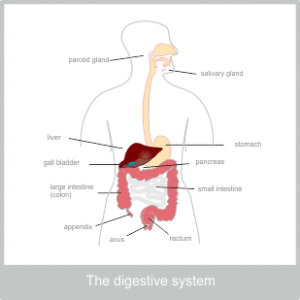
The Anatomy of the Digestive System
The Digestive system in primarily composed of an elaborate tube that runs from the mouth to the anus. This tube can be called the gastrointestinal or digestive tract, the alimentary canal or the gut. Along with a series of accessory organs, its role is to take in food and fluid, break it down into its component part, digest the useful constituents and discard and remove the rest. Water and nutrients that are released in the process pass through the walls of the digestive tract and move into the blood.
The Digestive tract is made up of distinct structures that are all design specifically for the role they pay in this process. They are the mouth, oesophagus, stomach, small intestine, large intestine and anus. Despite their differences, as part of essentially the same tube these structure do share the same basic components.
The entire digestive tract is made up of four layers. On the inside there are three layers collectively know as the mucosa, the inner most of these is called the mucous membrane. Mucous membranes are able to secrete mucus into the tract to lubricate and protect the cells from digestive enzymes. This layer is also able to absorb substances it comes in contact with. The inner most layer of the tract is replaced every few days. We can see the first part of the mucus membrane of the digestive tract inside our mouths.
Outside of the mucosa is a layer called the submucous layer, this contains enzyme producing glands, an intricate network of blood and lymph vessels, and an incredibly rich nerve supply, all within loose connective tissue.
The nerve supply in the digestive tract is focused in the submucosa layer but also extends into the muscles and the mucosa and has now been recognised by recent research, to function as an autonomous brain. With 500 million nerve cells inducing 100 million neurones of 20 different types, the Enteric Nervous System (ENS) as it is known, communicates with the emotional limbic system in the big brain and is in control of mechanical movement in the digestive tract, as well as chemical sensing leading to the release of enzymes and hormones. The ENS produces neurotransmitters (“molecules of emotion”) inducing 95% of the body’s serotonin which seems to indicate that we really do have ‘gut feelings’.
Nevertheless the brain does still have a part to play in digestion. On the whole parasympathetic nerves stimulate digestion and sympathetic (fight or flight) stimulation tends to shut it down. This is why stressful or frightening situations often feel like they affect our stomach.
Outside of this is the muscle layer. On the whole there are two distinct layer of muscle, the fibres of these two layers run perpendicular to one another, which increases their strength. On the inside the muscle fibres encircle the walls of the tube, while the outer one run along the length. Between the two there are more blood vessel, lymph vessels and nerves. Contraction and relaxation of these smooth muscles is called peristalsis. It moves food slowly along the digestive tract and also helps to mix food with digestive juices.
The outer layer of the digestive tract is called the adventita. For the upper section of the digestive tract this is a loose fibrous tissue but in the abdomen it forms the peritoneum. The peritoneum is the largest serous membrane in the body. Serous membranes secrete a watery fluid. It is made up of two layers, one that lines the abdominal wall and one that covers the abdominal organs forming a closed sac. The fluid it secretes fills the space between these layers and protects and lubricates the digestive tract so that everything can move smoothly in the abdominal cavity without friction, much like the pericardium of the heart and the pleura of the lungs.
The accessory organs of the digestive tract either open out or project into the hollow of the tube to aid the process of digestion. These are the tongue and salivary glands, the liver, pancreas, gall bladder and appendix. The salivary glands open via ducts in the mouth, the liver, gall bladder and pancreas all open via ducts into the top part of the small intestine and the appendix opens straight into the beginning of the large intestine.
The physiology of the digestive system
The Mouth to the Cardiac Sphincter
So now let us start at the beginning. The process of digestion begins in the mouth. The teeth, tongue and saliva work together with the muscles of the mouth to grind food up into a paste. Saliva is produced by three pairs of glands that are located in the face. One of these is in the outer cheeks, the other two are under the floor of the mouth and the bones of the jaw. They all have ducts that deposit the saliva in the mouth involuntarily. This process can be triggered by the sight, smell or even thought of food.
Saliva is important for several reasons. In the process of digestion saliva contains an enzymes called amylase that begins to break down cooked carbohydrates into saccharides (sugars). It also lubricates and cleans the mouth and keeps it moist and supple, as well as containing protective immune cells and clotting agents to defend against injury or attack. Saliva is also necessary to allow us to taste dry food as the taste buds only respond to particles dissolved in water.
However, the major organ of taste is the tongue, which is coated in specialised papillae that contain nerve endings that are sensitive to the four major tastes: sour, bitter, salty and sweet. As well as taste the tongue is designed to aid, chewing, swallowing and speech.
Moving down from the mouth we next come to the oesophagus. This runs from the back of the mouth down, behind the tubes of the lungs, to the opening of the stomach. At either end of the oesophagus there are sphincters that act as valves to control the flow of substances that travel along the tube. At the top a muscle ring at the end of the pharynx stops air from entering the oesophagus during breathing. At the bottom the oesophagus passes through the muscles of the diaphragm. It is here that the oesophagus begins to transform into the stomach and the muscles of the diaphragm act as a sphincter to stop the stomach contents from flowing back up into the oesophagus. This is known as the cardiac sphincter due to its proximity to the heart. It is at the level of the xiphisternal joint.
The Stomach
The stomach is a continuation of the oesophagus but acts like a holding zone for food. Due to the cardiac sphincter at its head and the pyloric sphincter at its base, it can close itself completely to form a sac. To complement the function of the Stomach, it also has an extra layer of muscle in its wall that run diagonally to the other two. This means that the stomach is able to churn more effectively when mixing and processing food.
Depending on what is eaten, food can remain in the stomach anywhere from 1 to 6 hours. Light fruit and vegetable meals will be there the shortest time, with heavy fatty meals there the longest. Once food enters the stomach hormones encourage the release of gastric juices via specialised glands that open into the stomach.
Gastric juices contain water, mineral salts, mucus, hydrochloric acid, intrinsic factor and inactive enzyme precursors called pepsinogens. The pH in the stomach can get as low as 1 and without the protective alkaline mucus lining the stomach would be severely damaged. However, this highly acidic environment is needed for several reasons. Firstly, it kills many microbes that have entered the body via food; secondly, it also allows minerals such as iron to be dissolved out of food and finally it plays a very important role in the digestion of proteins. This is because hydrochloric acid activates the inactive enzymes of pepsinogen to their active form, which is called pepsin. Pepsins begin the process of breaking proteins down into smaller part. Obviously this chemical conversion from inactive to active is extremely important because if the enzyme was produced in its active form it would digest the body itself, which is made up of protein.
Intrinsic factor is required for the absorption of Vitamin B12, although this does not happen until it reaches the small intestine.
The combined action of this chemical process and the mechanical churning and mixing of the stomach muscles leads to a liquefied substance called chyme. Very little is actually absorbed from the stomach, other than water, alcohol and some drugs.
The small intestine, pancreas, liver and gall bladder
From the stomach the tube of the digestive tract continues once more to transform into the small intestine. The small intestine is roughly 5 meters long and has an enormous surface area, due to its length and its convoluted structure. This makes it ideally suited to its major role of nutrient absorption.
Firstly, the inner walls of the small intestine form circular folds like a concertinaed pipe. Secondly, the walls of the mucosa layer are formed of tiny tentacles (approximately 1mm long) know as villi that project into the space in the tube like anemones. Furthermore, like fractals, every cell on the surface of these tentacles has its on tiny projections know as microvilli.
Each villi contains its own network of blood and lymph capillaries, to help it transfer nutrients to the rest of the body. If it could all be smoothed out, the surface area of your digestive tract would cover an astonishing 400m2!
The small intestine is divided into three distinct areas for descriptive proposes, the duodenum, the jejunum and the ileum.
The first part of the small intestine – the duodenum
The duodenum is about 23cm long. In the middle there is an opening protected by a sphincter (hepatopancreatic sphincter) This opening attaches to both the pancreas via the pancreatic duct and the gall bladder via the common bile duct. The pancreas, liver and gall bladder are all accessory organs of the digestive tract. We will discuss them here as this is the point at which they have their effect on the process of digestion.
The pancreas
The pancreas has two very important functions, one is as an exocrine glad, meaning it secretes into a localised area, and one as an endocrine gland – meaning that it secretes into the blood and therefore affects the whole body. (In this case the pancreas secretes the hormones insulin and glucagon to control blood glucose levels.)
Its exocrine function is to produce and store pancreatic juices. Pancreatic juices contain water, mineral salts, enzymes (amylase and lipase) and inactive enzyme precursors (trypsinogen, chymotrysinogen and procarboxypeptidase) Pancreatic juices are alkaline (pH 8) as is bile. When they mix with the chyme in the duodenum they raise its pH to around pH6-8.
In this case the inactive enzyme precursors are activated by an enzyme present in the microvilli and the intestinal juices, called enterokinase. Again they are then involved in the break down of proteins to amino acids, which is why they have to produce in an inactive form. Pancreatic amylase, continues the work of the salivary amylase and converts all available polysaccharides (starches) into disaccharides (sugars). Lipase converts fats into fatty acids and glycerol.
The gall bladder
The gall bladder is a small sac like structure that acts as a repository for concentrated bile produced by the liver. Bile is made up of water, mineral salts, mucus, bile salts, bilirubin and cholesterol. The bile salts are emulsifiers, which means they have the capacity to mix water and oil particles. This makes them useful for the digestion of fats as they can break fat down into smaller particles with a greater surface area. Bile salts are also required for the absorption of Vitamin K and digested fats. Bilirubin is a waste product of the breakdown of red blood cells. It is processed in the large intestine, with some parts being reabsorbed but most being converted to stercobilin, it is this that gives faeces its characteristic colour and smell.
The liver
The liver produces the bile that is stored in by the gall bladder and also process the end product of digestion that reach it through the blood. The liver is a very important and complex organ. Find out more here.
From the stomach the processed chyme is squirted into the duodenum through the pyloric sphincter. Depending on the contents to the food, this leads to a hormonal response from the lining of the duodenum, which encourage the release of bile and pancreatic juices. Along with these, the intestine also has its own juices. These contain, water, mucus mineral salts and the enzyme enterokinase. Around 3 litre of intestinal juices a day are secreted into the small intestine. Together all these various chemicals break down the chyme that has entered from the stomach into nutrients needed by the body. This process is finished within the cells of the villi, which means the end products are perfectly placed to be absorbed by the lymphatic system and the blood supply. This happen through both diffusion and active transport. Blood from the digestive tract travels into the hepatic portal vein and then on to the liver for further processing. As well as nutrients, the small intestine also reabsorbs over 8 litres of water a day.
The second part of the small intestine – The jejunum
The jejunum is the middle section of the small intestine and is around 2 meters long.
The third part of the small intestine – The ileum
The ileum is the last section of the small intestine where, fatty acids and the fat soluble vitamins they contain such as A, D, E and K, are absorbed along with vitamin B12 and the bile acids. The bile acids are returned to the liver where they are reused. Fatty acids and any vitamins that are dissolved in them are absorbed straight into the lymphatic system. The ileum is around 3 meters long. It converts into the large intestine at the ileocaecal valve which controls the flow of materials from the ileum to the caecum – the first part of the large intestine.
The large intestine
The large intestine is roughly 1.5 meters long. It is wider than the small intestine and forms and arch around the coiled up small intestine. Its structure differs slightly from the rest of the digestive tract as the muscles that run along its length are divided into three bands and are slightly short than the full length of the large intestine. This has the effect of puckering the organ a little. The large intestine also has considerably more lymphoid tissue, and more mucus secreting cells than the rest of the digestive tract.
The large intestine is also divided into several parts for descriptive purposes. These are the caecum, ascending colon, transverse colon, descending colon, sigmoid or pelvic colon, rectum ans anal canal.
The large intestine part one – The caecum and appendix
Caecum means blind end because it is just above this section of the large intestine that the small intestine attaches at the ileocaecal valve. This makes the caecum and the appendix at the base of it a bit like a U bend in a sink. The appendix is approximately 13 cm long.
The large intestine part to – The ascending colon
The ascending colon is the section of the colon that travels up from the ileocaecal valve to the level if the liver where it bends acutely to the left forming the hepatic flexure.
The large intestine part three – The transverse colon
From the hepatic flexure the next section of the large intestine is known as the transverse colon due to its direction of travel. It travels across the abdomen in front of the gall bladder, duodenum, pancreas and stomach, right the way over to the spleen. At this point it bends down again at the splenic flexure.
The large intestine part four – The descending colon
The section of the large intestine that travels down from the splenic flexure in known as the descending colon. As is travels downwards, it curves in towards the midline.
The large intestine part five – The sigmoid or pelvic colon
When this section enters the pelvis it is known as the sigmoid colon. This is an s shaped section of bowel that moves around the bony structure of the area. At this point the muscles that run the length of the colon become continuous again, reverting back to the general plan of the digestive track. This gives us more muscle control for evacuation.
The large intestine part six – The rectum
The rectum is a continuation of the sigmoid colon and is about 13 cm long. At this point the large intestine becomes wider
The large intestine part seven – The anal canal
The rectum terminates in the anal canal, which is the exit route of waste material into the outside world. The anal canal is about 4cm long in an adult and ends at the anus itself. This is made up of two sphincters, the internal and external anal sphincter.
When food that has passed through the rest of the digestive tract enters the large intestine, the process of digestion that up until now has been largely chemical, switches to being predominately biological. This is because the large intestine is home to millions of microbes including bacteria and yeasts. Although some of these may be harmful to us in other context, in the bowl they work symbiotically helping us to synthesise important chemicals such as vitamin K and folic acid.
Recent work by the Human Microbial Project, sequencing the DNA of human microbial populations is beginning to show how hugely important these tiny inhabitants are. They outnumber our cells 10 to 1 and are now thought to be involved in the development of and protection against disease, our individual rates of our metabolism and possibly even our behaviour. The latest research suggests although there are huge variations between the microbes of individual people, four distinct microbial populations can usually be identified. These are oral, skin, faecal and vaginal (which we all get from our mothers during normal birth). Of these the faecal population is the most complex making Large Intestine the largest potion of our immune system.
Gas can also be present in the digestive tract. This can come from air that is swallowed during eating or drinking. However, hydrogen, carbon dioxide and methane may also be produced by biological fermentation of unabsorbed nutrients, especially carbohydrates, in the large intestine. These gases pass out as flatus. As well as the products of biological break down the large intestine also absorbs, mineral salts, some vitamins and drugs and the majority of the water left in the substances. This leads to the semi solid consistency of faeces.
The large intestine is not moved by the normal peristaltic action of the rest of the digestive tract. In the large intestine, muscular waves of movement happen much less frequently and are characteristically precipitated by food entering the stomach. This leads to a process know as mass movement, where the contents of the large intestine are forced into the sigmoid colon and rectum. This process is known as gastronomic reflux.
Once mass movement has forced faeces into the rectum, nerves that are sensitive to stretch, alert us to the need to defecate. As with the bladder, in babies this leads to a reflex action which is not under voluntary control. However, as the nervous system matures we learn to control this reflex so that we can find a convenient time to defecate. However, if we resist the urge the feeling of fullness is likely to fade until the next mass movement. If we repeatedly suppress the reflex, we may become constipated.
Faeces
The faeces that leaves the body is made up of water, fibre, dead and live microbes, epithelial cells from the walls of the digestive tract, fatty acids and mucus secreted by the large intestine to lubricate its movement. Its characteristic colour comes from stercobilin.
Sources
Ross and Wilson – Anatomy and Physiology
https://www.amazon.co.uk/Wilson-Anatomy-Physiology-Health-Illness/dp/0702053252/ref=sr_1_1?ie=UTF8&qid=1454518424&sr=8-1&keywords=ross+and+wilson
The complimentary therapist guide to conventional medicine – Dr Clare Stephenson
http://www.amazon.co.uk/Complementary-Therapists-Guide-Conventional-Medicine/dp/1848193076/ref=sr_1_1?ie=UTF8&qid=1454518461&sr=8-1&keywords=clare+stephenson
Wholistic Anatomy – an integrative guide to the human body – Pip Waller
http://www.amazon.co.uk/Holistic-Anatomy-Integrative-Guide-Human/dp/1556438656/ref=sr_1_1?ie=UTF8&qid=1454518495&sr=8-1&keywords=pip+waller
TED talk: How our microbes make us who we are – Rob Knight
http://www.ted.com/talks/rob_knight_how_our_microbes_make_us_who_we_are
TED talk: The brain in your gut – Heribert Watzke
http://www.ted.com/talks/heribert_watzke_the_brain_in_your_gut
TED talk: Meet your microbes – Jonathan Eisen
http://www.ted.com/talks/jonathan_eisen_meet_your_microbes
Candice Pert – Molecules of Emotion: Why you feel the way you feel
http://www.amazon.co.uk/Molecules-Emotion-Why-You-Feel/dp/0671033972/ref=sr_1_1?ie=UTF8&qid=1454518387&sr=8-1&keywords=molecules+of+emotion